




B12 Deficiency is a Silent Epidemic That is Routinely Missed and Under-Diagnosed.
Have you ever had a “senior moment?”


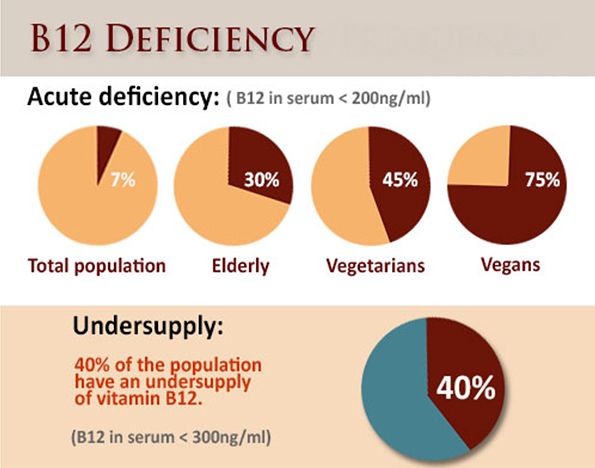
Consider this: an estimated 40% of people over 60 years old are deficient in B12, which leads to cognitive decline, memory loss and even Alzheimer’s and dementia.
We’ve accepted that a significant decline in our cognitive
abilities is just part of getting older, when in many cases it may be something
as simple as not getting, or absorbing, enough of the right kind of B12.
- Why is B12 deficiency so under-diagnosed?
- Why does one study show that over 80% of
vegans lack sufficient B12?
- Do you have to wait until your symptoms are
serious, or even life threatening, to find out if your B12 is too low?
- Why do so many people have trouble absorbing
B12?
- Did you know you can’t get it from plants?
What Everyone
(Especially Vegetarians) Should Know About B12 Deficiency.
Do you know which foods are the best sources of B12?

Here’s a hint: studies consistently demonstrate that up to 50% of long-term vegetarians and 80% of vegans are deficient in B12. B12 is the only vitamin that contains a trace element (cobalt), which is why it’s called cobalamin.
Cobalamin is produced in the guts of animals, and is the only vitamin we can’t obtain from plants or sunlight.
Plants don’t need B12, so they don’t store it.
A common myth amongst vegetarians and vegans is that it’s possible to get B12 from plant sources like seaweed, fermented soy, spirulina and brewers yeast.
But plant
foods said to contain B12 actually contain B12 analogs called cobamides that
block absorption of and increase the need for true B12.
Even on the Paleo
Diet, it is Possible to be Deficient in B12.
Even if you eat
meat 2-3 times per day, there are still many things that can interfere with
absorption of B12.
This is a case where it is better to be safe than sorry. B12 depletion can take years to become clinically evident
i.e. B12 deficiency sets in long before obvious symptoms appear
Some of the more serious effects of B12 deficiency (such as nerve
damage) are irreversible.
One of the greatest tragedies of the B12 epidemic is that diagnosis and treatment is relatively easy and cheap –
Especially when compared to treatment of the diseases B12 deficiency can cause

So should you be
concerned? Well, some people are at greater risk than others.
- vegetarians and vegans
- people aged 60 or over
- people who regularly use PPIs or acid
suppressing drugs
- people on diabetes drugs like metformin
- people with Crohn’s disease, ulcerative
colitis, celiac or IBS
- women with a history of infertility and
miscarriage
Whether or not you
are included in the list above, everyone concerned with good health should
understand the basics of this silent epidemic.
B12 deficiency is often missed for two reasons.
First, it’s not routinely tested by most physicians.
Second, the low end of the laboratory reference range is too low.

This is why most studies underestimate true levels of deficiency.
Many B12 deficient people may have so-called “normal” levels of B12.
One of the biggest problems with diagnosing B12 deficiency is that the conventional serum B12 test that most doctors run only picks up a small fraction of people who are actually B12 deficient.

The test measures the total amount of B12 in the blood, and
does not rule out functional B12 deficiency.
The next time you or someone you know is “having a senior moment,” remember: it might not be “just aging.” It could be B12 deficiency.

Metabolic
vitamin B12 deficiency: a missed opportunity to prevent dementia and stroke
Abstract
The purpose of this
narrative review is to highlight insights into the importance and frequency of
metabolic vitamin B12 (B12) deficiency, reasons why it is commonly missed, and
reasons for the widespread but mistaken belief that treatment of B12 deficiency
does not prevent stroke or improve cognitive function.
Metabolic B12
deficiency is common, being present in 10%-40% of the population; is frequently
missed; is easily treated; and contributes importantly to cognitive decline and
stroke in older people.
Measuring serum B12
alone is not sufficient for diagnosis; it is necessary to measure
holotranscobalamin or functional markers of B12 adequacy such as methylmalonic
acid or plasma total homocysteine.
B-vitamin therapy
with cyanocobalamin reduces the risk of stroke in patients with normal renal
function but is harmful (perhaps because of thiocyanate accumulation from
cyanide in cyanocobalamin) in patients with renal impairment.
Methylcobalamin may
be preferable in renal impairment.
B12 therapy slowed
gray matter atrophy and cognitive decline in the Homocysteine and B Vitamins in
Cognitive Impairment Trial.
Undiagnosed metabolic B12 deficiency may be an important missed opportunity for prevention of dementia and stroke.
In patients with metabolic B12 deficiency, it would be
prudent to offer inexpensive and nontoxic supplements of oral B12, preferably
methylcobalamin or hydroxycobalamin.
Future research is
needed to distinguish the effects of thiocyanate from cyanocobalamin on
hydrogen sulfide, and effects of treatment with methylcobalamin on cognitive
function and stroke, particularly in patients with renal failure.
Plasma total
homocysteine increases at serum B12 levels less than 300-400 pmol/L.
Only 26% of
patients referred to a stroke prevention clinic had serum B12 levels greater
than 400 pmol/L.
Among patients with
serum B12 in the borderline range, tests of functional B12 such as
holotranscobalamin, methylmalonic acid, or (in folate-replete patients) plasma
total homocysteine are necessary to exclude metabolic B12 deficiency.

In This eBook You’ll Learn
- The early symptoms of B12 deficiency that are going undiagnosed in most people
- How B12 deficiency is commonly missed or misdiagnosed
- What B12 is, how it works and why you need it
- The best sources of B12
- What may be preventing you from absorbing the B12 you are getting
- Whether you are deficient in B12
- How often should you test
- What you should do if you discover that your B12 is low
